Quaderns de Psicologia | 2022, Vol. 24, Nro. 2, e1821 | ISNN: 0211-3481 | ![]()
 https://doi.org/10.5565/rev/qpsicologia.1821
https://doi.org/10.5565/rev/qpsicologia.1821

Trajectories towards affirmation: Gender identity in mental health services after the ICD-11
Trayectorias hacia la afirmación: La identidad de género en los servicios de salud mental después del CIE-11
Konstantinos Argyriou
Spanish National Research Council
Autonomous University of Madrid
Abstract
Depathologisation of gender diversity in the ICD-11 marks a shift in psychological services for transgender and gender nonconforming people. Even though the stipulated changes are only practically applicable ever since early 2022, a general move towards affirmative psychotherapeutic and counselling practice has been noticed ever since 2018. The present paper covers three main models of mental health care for gender minorities, namely the conversion therapy model, the transsexual gatekeeping model, and the affirmative model, in order to view them under a novel lens. Drawing on Science, Technology and Society Studies, the universalist presumptions and rigid gender roles of the traditional models are brought under scrutiny. Moreover, the itinerary reveals the need for situated narratives that encourage self-determination and renovate the therapeutic relationship as a means of self-exploration instead of an institutional control mechanism. Concluding, it is remarked that intersectional knowledge is crucial in compensating for micro-aggressive practices and dynamics historically promoted by psychologists and other mental health providers.
Keywords: Counselling; Psychologists; Gender identity; Situated knowledge
Resumen
La despatologización de la diversidad de género en el CIE-11 marca un giro para los servicios psicológicos para personas trans y no conformes al género. Aunque los cambios estipulados solo se incorporan prácticamente desde principios de 2022, se ha estado observando un movimiento general hacia la práctica psicoterapéutica y de asesoramiento afirmativo desde 2018. El presente artículo realiza un recorrido por los tres modelos principales de atención de salud mental para minorías de género, concretamente el modelo de terapias de conversión, el modelo transexual de vigilancia, y el modelo afirmativo, con el fin de contemplarlos bajo una nueva perspectiva. Partiendo de los Estudios de Ciencia, Tecnología y Sociedad, se examinan las presunciones universalistas y los roles rígidos de los modelos tradicionales. Además, el recorrido revela la necesidad de narrativas situadas que incentiven la autodeterminación y renueven la relación terapéutica como eje de autoexploración en vez de mecanismo de control institucional. Como conclusión, se remarca que el conocimiento interseccional es crucial para compensar las prácticas micro-agresivas y dinámicas que históricamente han promovido psicólogos y otros prestadores de servicios de salud mental.
Palabras clave: Asesoramiento; Psicólogos; Identidad de género; Conocimiento situado
Introduction
Since the official depathologisation of trans identities in the latest version of the International Classification of Diseases (ICD-11) (Castro-Peraza et al., 2018; 2019), little is known regarding the impact of the historical change on psychotherapeutic and counselling practice. In various public services worldwide, participation of mental health care providers (MHPs) has already been lessened or suspended, since their involvement in healthcare provision is not considered obligatory anymore (Gómez-Gil et al., 2020; Spanos et al., 2020).
This rearrangement cannot be directly attributed to the only completely effective in early 2022 ICD revision (Gaebel et al., 2020). Instead, it involves a general tendency towards citizen participation and self-determination in mental healthcare of gender diverse people (Ortega Arjonilla et al., 2018). It cannot be easily documented, either, since services of the kind are not offered by single entities but by several institutions of different calibre, including Gender Units of University Hospitals, primary health centres, private practice, LGBTQI organisations, and others. Moreover, MHPs perform a variety of tasks depending on their abilities and context. Psychotherapy and counselling are different procedures themselves, entailing different sets of methods, usually for different purposes. Here they are examined jointly, along with psychological assessment, as mental health services (Wylie et al., 2016).
Before the ICD revision and despite its own predicaments (see Suess, 2020, for a criticism), dominant biomedical, psychological and legal discourses had been promoting a Western, dichotomous, normative model of understanding gender (Fausto-Sterling, 2000; Johnson, 2016; Spade, 2006). This model, replete with universalist assumptions, has been grounded upon the entitlement of those discourses to granting legitimacy to certain prototypical identities, and to imposing and institutionalising normative positions as natural, through laws, tax rules, or values such as monogamy (Athanasiou and Butler, 2013; Iantaffi and Bockting, 2011; Sennott, 2010). Gender role expectations have constituted a quantitatively measurable artefact (López-Sáez and García Dauder, 2020) with painful implications for people who do not fall within this traditional gender dichotomy (Doan, 2010). Therefore, psychological practice has contributed to the erasure of alternative testimonies, narratives, and modes of conceiving sex and gender (Bauer et al, 2009; Occhino and Skewes, 2020).
Transgender and gender non-conforming people1 are notably more likely to seek mental health services for gender issues than the rest of the LGTBQI community is for issues related to sexual orientation and sexual identity (Hendricks and Testa, 2012; Israel et al., 2008). They are also more likely to find those services unhelpful or ignorant of their particular needs (Benson, 2013; Suess, 2020). Psychotherapy’s ineffectiveness and subjects’ dissatisfaction have often been reported both in literature and throughout empirical studies (Bockting et al., 2004; Raj, 2002). This negative relation has led to a history of mutual suspicion, where subjects have had to assume the training role, due to a generalised lack of specific training on LGBTQI issues in mental health providers’ curricula (Carroll and Gilroy, 2002; Chavez Korell and Lorah, 2007; Gherovici, 2017).
In psychotherapy and counselling with TGNC people, Patrick Grzanka and Joseph Miles (2016) document three main models: the conversion model (or pathologisation), the gatekeeping model (or incorporation), and the affirmative model (affirmation). Each model supposes a different approach to the therapeutic relation. It is significant to observe how this threefold division has configured the therapeutic space during the last two decades, and how shifts in psychological practice have affected power relations between MHPs and gender diverse clients. Additionally, such division is neither merely chronological, nor a simple mimicking of ICD revisionist culture: the three models may even coexist over time, creating a complex landscape of practices. There is, however, a linear evolution in terms of renouncing institutional violence, the affirmative model being the most inclined towards reading gender dysphoria as societal prejudice instead of an individual issue (Tosh, 2016).
I purport to use the aforementioned division to examine the universalist presumptions behind TGNC experiences that have perpetuated this culture of suspicion. Although I endorse their call for epistemic break from positivist and post-positivist paradigms (Tosh, 2016, p. 376), I depart from their invitation to actualise psychological work by forcing it out of the therapy room (Tosh, 2016, p. 386), proposing a novel, critical examination of the therapeutic relation instead. My aims are to explore how specific dynamics between TGNC people and psychologists are affected by dominant psychological discourses that have promoted universal, standardised ideals of transgender identity; and subsequently, to contemplate the changes brought by the recent ICD revision.
In order to examine the discursive and contextual aspects of subjective formation that cannot be revealed through standard psychological and taxonomical technologies, I appeal to studies that address the therapeutic alliance. Grzanka and Miles believe that Science and Technology theorists have not sufficiently stipulated gender identity issues in psychotherapy, leaving knowledge production in the field to be assumed almost entirely by psychologists (Grzanka and Miles, 2016, p. 372). I use the situated knowledge acquired through feminist and critical STS (Campbell, 2009; Latham, 2016), to understand alliance itself as a technology of narrating, exploring and configuring gender. Gender identity emerges in therapy through practises and narratives of diverse value, depending on each particular cultural and professional context.
Throughout the text, I do not consider psychotherapeutic accompaniment incompatible with gender self-determination. Even though the notion of gender configuration implies a dyadic process, where the psychotherapist or counsellor reflects certain aspects of the person’s gender identity back to them, that does not a priori constitute monitoring. Accompaniment of TGNC people may not concern their gender identity, but rather issues of exclusion, discrimination, stigma and well-being (Benson, 2013; McBee, 2013). Accordingly, under no circumstance should psychotherapy itself be understood as a forceful practise of aversion or of “curing” trans people, unless when explicitly referring to conversion therapies.
Overview: A history of following the stereotype
Transgender identities and experiences are utterly disparate, bringing to the surface not only the discordance between gender identity and sex assigned at birth, but more importantly, what gender identity is about: social group membership, felt contentment with one’s own self-presentation, felt pressure for conformity, and attitudes towards other gendered groups (Egan and Perry, 2001; Wood and Eagly, 2015). TGNC people in Western societies have long been obliged to comply with several psychiatric, medical and legal criteria of gender in order to be recognised as such and be relatively integrated into society (Billings and Urban, 1982; Hines, 2013; Johnson, 2016). Passing, the “ability” to socially hide trans status (Garfinkel, 1967/1991), has been a key element in this system of compliance.
As a standpoint of societal power distance, passing creates a double paradox, since it signals that both by passing as non-transgender (from now on, cisgender) and by failing to do so, TGNC individuals are flawed (Spade, 2006). In case they pass as members of dominant gender groups (men or women), apart from the high levels of self-policing they need to submit themselves to, they are frequently met with distrust and hostility. Society might react by believing TGNC people have misleading behaviours or are even lying about themselves. In case they fail to pass, they seem to be “doing gender” in an unsuccessful way. In both cases, they are being thought of us deceivers. Thomas Billard (2019) has called this framework “the deception frame”.
Under these circumstances, it would seem fundamental to examine whether a person followed gender norms correctly, by dressing, talking, moving and behaving in a standardised, stereotypic mode. Therefore, gender evaluation was a task many MHPs would implement (Serano, 2016). Sandy Stone (1987/1991) was one of the first theorists to elaborate on how TGNC people who wished to receive hormonal treatment or to undergo “sex reassignment surgery” would study referential texts, get informed by other testimonies and follow professional guidelines in order to perfectly match established transition criteria. Gender evaluation was an obstacle to overcome, a challenging but inevitable play one had to assume, if they wanted to accomplish bodily modification.
Professionals’ “determining gender” has been in constant dialogue with subjects’ “doing gender”. Determining gender is a term that signals how our gender identity is authenticated or assigned by others, through our expressions, presentations and behaviours (Westbrook and Schilt, 2014). Psychological practise has played a major role in configuring this external representation, with direct effects to TGNC people’s self-perception (Tate, 2014). MHPs would reflect their “standards of gender” and would validate a certain narrative that “did gender” via pre-approved standards. Gender evaluation was attached to a gatekeeping role that wished to ensure identity stability through time and erase the fear of regret of surgical interventions. In this asymmetrical dynamic, therapists desired to hear that the lust for change came from desperation and dissatisfaction (Latham, 2016; Spade, 2006). Even until our days, verbal scales of masculinity and femininity might still avow for such kind of performances (López-Sáez and García Dauder, 2020).
In another important account, Douglas Mason-Schrock (1996) informs of the narrative constitution of the “true self” within transgender support groups. At least until the 1990s, personal stories of members would be submitted to intragroup revisions in order to conform to a standard ideal of transsexuality. In fear of losing recognition, groups would be tactfully blind to internal contradictions of new members’ narratives, and would instil the storylines they would find more appealing. Members would be guided towards essentialist narratives (for instance, memories of cross-dressing in childhood), because socially constructed transsexuality would be subject to contempt.
This wrong body narrative implicitly validated the existence of a right body experience, and ascribed gender dysphoria exclusively to transsexual people (Halberstam, 1998; Hausman, 1995). Initially popularised during the 1960s, it was revolutionary in terms of dismissing a traumatic tradition of conversion therapies. Nonetheless, in the 1990s it was beginning to seem insufficient, since an increasing amount of TGNC people would claim their independency from the strict criteria of the biomedical and psychiatric system and would define themselves as trans even without any need of bodily intervention. Activist groups, radical thinking on gender, and distrust on health professionals’ motives, initiated a process of gradual alienation from the narratives Mason-Schrock and Stone describe. The shift, however, seemed like a threat to those people who depended on the system’s confirmation in order to fully transition, and that mounted to a series of conflicts inside the transgender community (Johnson, 2016; Missé, 2018).
The tensions between the transsexual and the transgender model (Denny, 2004) have direct analogies with the tensions between the wrong body narrative and the narrative of gender affirmation, both of which describe forms of speaking about being trans, although these parallelisms are neither secured nor absolute. Gender affirmation (Ehrensaft, 2012; Grzanka and Miles, 2016; McBee, 2013) emerged as a counter-paradigm to strict understandings of gender norms. Instead of viewing masculinity and femininity as the only existent forms of gender legitimacy, opposite, complementary, and highly portrayed, this new model would permit divergent expressions of gender. A new path was being opened for nonconforming, nonbinary and agender people, who discovered new means of defining themselves, but would still have to fight against society’s narrow gender definitions.
The transgender model was more permissive and explorative, and gender affirmation was far more liberating than the protocols of conventional gender evaluation and personality assessment. It posed issues the normative society was unwilling to face: how were legal documents, health services and gendered spaces, supposed to adapt themselves to alternative understandings of gender categories? Once again, recognisability would bring to the surface a culture of mutual suspicion and distrust, but this time, the basic difference was that approaches to gender diversity would be more client-centred and individualised, based more on bodies and less on protocols (Bockting, 2008; Carroll and Gilroy, 2002; Raj, 2002). Trans rights bills and the inclusion of TGNC people in the public sphere still followed the binary, activating gender panics whenever boundaries seemed to be shaken (Rood et al., 2016; Westbrook and Schilt, 2014).
Online culture arrived after the 1990s as another catalyst, by breaking both with a system of well secluded expert knowledge and with an idea that there is a unique pre-established way to “make transgender identities”. Many internet users started sharing, comparing, and discussing their experiences in health care, both physical and mental. Many others solicited hormones in illegal markets, arranged transition package trips to foreign countries, or simply met with people they would find in forums and associations (Raun, 2014). This culture of globalisation and instant sharing had both advantages and disadvantages: it brought power to citizen participation while also making transgender presences more homogeneous. The drawbacks of annihilating internal contradictions and rich variance in the support groups of the early 1990s, were also noticed in the commercial ways of presenting trans lives through the internet.
On the whole, the divisions between expert and lay, legal and illegal, global and local knowledge began to blur with the shift towards the new Millennium. Only after two decades into the 21st century can they be clearly appreciated, however. Even though psychological theory and practice have adapted to new gender schemes, at times not without resistance, the evolution has only been progressive and following activist claims, not preceding them. Moreover, as shall be seen below, psychological associations have generally altered their representations and attitudes towards gender diversity with time, at least in Western contexts (see APA, 2015; BPA, 2019), whilst psychiatric organisations maintain a more cautious approach to questioning the binary. The latest version of the DSM-5 (2013) can confirm such retardation. Given the spatial and historical contingencies of gender roles, the issue of cultural adaptation of guidelines is still largely pending.
Analysis: Tracing the prevailing models
Trans identity is neither transgressive nor conservative by definition (Halberstam, 1998). Some TGNC people bodily transition to achieve passing and acceptance as members of the two dominant gender groups, while others consider their transition a political move. Similarly, psychology remains relatively divided into trans-friendly and trans-sceptical approaches, although orthodox psychoanalytic or behaviourist theories are increasingly getting marginalised. A fundamental task of critical approaches concerns detecting the positionality and situated enunciation of each study or counselling practice. Nonetheless, there are various border wars that require further conceptualisation. Lisa Burckell and Marvin Goldfried (2006) establish a spectrum of five therapeutic approximations, verging from exclusionary therapist characteristics to essential alliance facilitation traits, while Jack Drescher (2013) and Grzanka and Miles (2016) simplify them to three positions, as described earlier, leaving less intermediary space.
The therapeutic space is a private, confidential space, and as such it configures gender differently than public, quasi-public and semi-private spaces do (see Westbrook and Schilt, 2014 for an analysis of space). It is a place supposedly defiant of surveillance and intrusion, or of what Petra Doan calls the tyranny of gender (Doan, 2010), although therapeutic perspectives play a decisive role regarding this aspect (Mizock and Lundquist, 2016). The way gender is performed inside a therapeutic session is conditioned upon the dynamic between performer and receiver, but also upon the material space that surrounds them. For instance, MHPs can rely on the public/private divide in order to remain discreet about their personal emotions (Fernández Garrido, 2021). Similarly, their own gender identity negotiation can be concealed through focusing on the nonnegotiable distance between them and the clients, both metaphorically and physically.
Alliance is usually established in the beginning of the therapeutic relationship, when the demand is enunciated and initial boundary negotiation takes place. Microaggressions are subtle communicative cues that discriminate against vulnerable populations, including TGNC people, and have the capacity of damaging this alliance. Misgendering, the use of inappropriate gender pronouns when addressing a TGNC person, and deadnaming, the tendency to use a TGNC’s name assigned at birth instead of their chosen name, are major signs of lack of training on issues of gender diversity. Both micro-aggressive behaviours can be unconscious or deliberate (Clark and Loewenthal, 2015; Freeman and Stewart, 2019; Nadal et al., 2012).
These attitudes are determining of alliance even from the first session (McLemore, 2014). Alliance here is to be understood as a slightly broader notion from trans or LGBTQI allyship, since the former refers to the process of creating emotional rapport between psychotherapist and client, while the latter focuses on advocacy. In practice, TGNC clients deduce allyship through alliance. An impaired therapeutic alliance is the main reason why a person would change their psychotherapist, while alliance is particularly low in cases of involuntary referral. Moreover, a less engaged alliance may indicate a higher dependency on psychometric evaluation in order to substitute for the lack of provided information or emotional rapport (Burckell and Goldfried, 2006). That is not to say that tests are exclusively of compensatory use when the relation is deficient; they might, however, operate as mediators when clients resist disclosure.
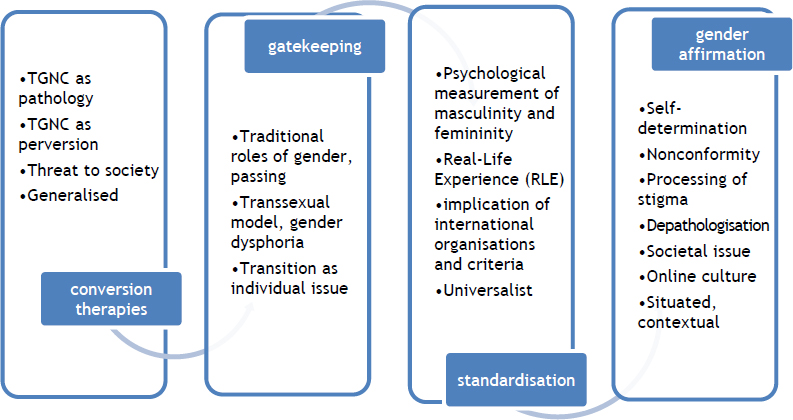
Figure 1. The narrative shift towards gender affirmation
Conversion therapies
Keeping those preliminary accounts in mind, I shall proceed to the model analysis. The model preceding the transsexual gatekeeping model, not necessarily chronologically but mostly in terms of sophistication, is that of conversion therapies (alternatively, reparative or aversion therapies). The model neither informs a culture of suspicion, nor is considered scientific; thus my mention will be restricted.
In the conversion paradigm, people are not asked to comply with any rules or standards, and their lived experience is rarely taken into account in what concerns their gender identity and expression (Israel et al., 2008). In undergoing conversion therapy, clients are obliged to accept the therapists’ idealisation of cisgenderism and heterosexuality as the only viable way of gender subjectivation (Drescher, 2007). Conflation between gender identity and sexual orientation under the scope of psychopathology is persistent and non-negotiable, while culpability and moral degradation become the main methods through which stigma is internalised (Tosh, 2016).
Furthermore, therapeutic techniques are hardly specified in studies that employ conversion therapy, some of which entail pastoral doctrines. In a review by Wright et al. (2018), results would rely mostly on therapists’ interpretations, rather than on clients’ subjective accounts, and would not have any longitudinal value. Harm, both primary and secondary, would therefore seem inevitable, since the coercive mechanisms used by defenders would include judgement, misgendering, interventionism and lack of compassion for TGNC experiences. Although conversion therapies have been banned by Western psychological practice (Grzanka and Miles, 2016), gatekeeping and barriers to healthcare access represent their understandable remainder. In line with this, crosscultural information on conversion practices is still scarce, as most related studies maintain a homogeneous perception of culture.
Gender evaluation in the transsexual gatekeeping model
The same mechanisms that historically served to legitimise certain identities and practices under the transsexual model were used by MHPs, in order to legitimise diagnostic labels as objective and neutral (Sennott, 2010; Serano, 2016; Tosh, 2016). One of those mechanisms was the compliance between the two prevalent diagnostic manuals, the ICD and the DSM (Drescher, 2013). Another one, as has been outlined, was the prevalence of binary gender categorisation (Lugones, 2008).
For that purpose, the transsexual gatekeeping model determines gender in the therapeutic encounter by incorporating the wrong body narrative both through structural (societal) and applied (professional) mechanisms. This is not to sustain that psychology and psychotherapy are exempt of responsibility in having assumed a monitoring role in the history of this dynamic, but rather to highlight that the majority of discourses displayed in clinical practice have pertained to biomedical relocations and indications of how gender identity should be perceived. Psychologists form a generally more permissive community of practitioners compared to other MHPs (Pingitore et al., 2002). Their authority, however, might be manifested through uninformed discriminatory acts.
Lived experiences of prejudice are not commonly acknowledged in the therapeutic alliance of the gatekeeping model, while secondary traumatisation is a potential threat (Freeman and Stewart, 2019; Nadal et al., 2012; Raj, 2002). For instance, Kevin McLemore (2014) describes three commonplace misgendering practices: using incorrect gender pronouns to address a TGNC person, gendering neutral and nonbinary names, and judging individuals for their “failure to pass”. Misgendering can also occur through gendered references to biology, for instance to chromosomes or hormones (García Dauder, 2018). Apart from misgendering, common emotional and epistemic misconduct includes universalising and exoticising trans experiences, denial of structural prejudice, disapproval, gaslighting, harassment, denial of trans people’s privacy and pathologisation (Freeman and Stewart, 2019; Mizock and Lundquist, 2016). Considering contextual factors is fundamental in the detection of microaggressive behaviours and of anticipatory stigma (Nadal et al., 2012).
Gender identity evaluation, although scarcely verbalised as such, consists of the following (also see Bockting, 2008):
-Administration of batteries of psychological tests (long-scale psychometric personality inventories, projective assessments, clinical interviews);
-Lifestyle surveillance (hormonal doses, habits);
-A strict 6-month to 2-year procedure called “Real-Life Experience” (RLE), where people would be obliged to present themselves according to their “desired” gender, performing the role in order to gain credibility in front of the mental health care provider.
Meanwhile, MHPs of the model follow agreed-upon guidelines and protocols, instead of personalising their services, and insist on a “checklist” rationale of evidencing rehearsed narratives. They therefore assume a paternalistic role, rather than an authentic, horizontal, permissive one, and usually avoid accompanying people with fluid and nonconforming gender expressions, in fear of being accused of complicity, in cases of regret (Stone, 1987/1991). Standardised personality inventories measuring masculinity and femininity sometimes substitute clinical interviews, assisting the maintenance of the dichotomy expert-lay person (López Sáez and García Dauder, 2020; Tosh, 2016).

Figure 2. Characteristics of the transsexual gatekeeping model
Aspirants to gender confirmation therapy would be conscious of the compelled fictions to which they were submitted, unlike Hausman’s argument that they were the biomedical system’s complacent victims. This is the main reason why feigning seems to substitute therapeutic alliance in the Real Life Experience: clients fear that authenticity and self-disclosure could infringe the standardised assessment routines of “true transsexualism”.
Shifting from the culture of suspicion to the affirmative model
Large part of the withdrawal from the gatekeeping model can be attributed to the understanding that minority stress TGNC people face is more responsible for their distress than their personal distress or a possible pathology (Ehrensaft, 2012; Gerritse et al., 2018). Nonetheless, simple realisation has not proved sufficient. As Judith Butler states, “when an authority is asked to recognise someone as trans, this authority is at the same time asked to transform their own understanding of gender, desire and the body” (2010, p. 7; translation is mine).
The paradigm change has been brought with the introduction of the affirmative, depathologising model, based on not questioning people’s gender identity (Missé, 2018). Affirmation is the accompaniment in combating distress caused by societal pressures for conformity. The model avoids test administration, pathologisation, and other acts of gender surveillance, allowing for experimentations, fluidity, and resistance to gender norms.
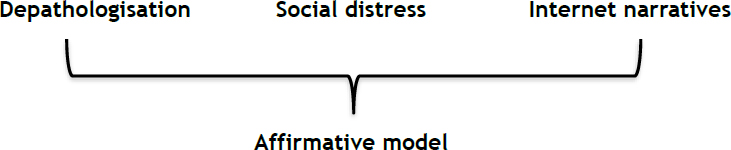
Figure 3. Characteristics of the affirmative model
Affirmative and person-centred approaches to psychotherapy are currently experiencing massive expansion, as a response to still prevailing vertical biomedical technologies. Switching to accompaniment, these approaches conciliate expertise with lived experience, thus providing hybrid, horizontal and bidirectional knowledge (García Dauder, 2018). Lay social movements have assisted the evolution from one-dimensional views of sex and gender to kaleidoscopic ones. Affirmation emerges as a trans-theoretical approach to cultural competency, instead of claiming to establish a separate therapeutic model. Even though hard to operationalise, it refers to the therapists’ acquisition of knowledge and awareness of the unique challenges LGBTQI+ subjects face in their lives, and the translation of this awareness to concrete counselling skills (O’ Shaughnessy and Speir, 2018). Awareness begins by reviewing generalised assumptions and personal biases against gender diversity.
Diane Ehrensaft (2012) suggests a multifactor bio-psycho-social development of gender identity, focusing on the Winnicottian transitional space and on children with variant gender expressions (Ehrensaft, 2012). She also highlights that terminology is a relentlessly slippery and creative issue, since it is when we think we have conquered linguistic novelties that they may become obsolete. Selfassignation of gender identity is highly contextual and depends on various cultural, linguistic and socioeconomic factors (Tate, 2014).
Affirmative alliance (O’ Shaughnessy and Speir, 2018) is the coalition that accepts the self-defined form of the person’s identification (name, pronouns), while providing strategies to counter cis-normative discrimination. It allows questioning internalised prejudice in clinical practise, emphasising how social judgements may get confounded with clinical ones, and how to overcome secondary stereotyping (Clark and Loewenthal, 2015). An important reason why affirmative competency is recommended is that therapists may not necessarily be aware of their clients’ minority status, but should still be able to detect the unique challenges associated with it (Israel et al., 2008). As aforementioned, this shift to a more consultant and advocating role, in association with critical psychology and STS approaches to affirmative practice (Clark and Loewenthal, 2015; Grzanka and Miles, 2016) affect the therapists’ stance and demand a new positioning.
Moving towards local, situated knowledge
However obvious it might seem that psychologists who assess TGNC people must be properly trained, well informed and responsive to their needs, affirmative understanding depends on legislative definitions and socio-cultural perceptions of gender, general attitudes towards gender minorities, as well as psychotherapeutic approaches. Self-definition is dependent on social connotations of masculinity and femininity: the more heteronormative the context, the greater the power distance is between a TGNC and a cis person that both define themselves as women (Westbrook and Schilt, 2014). Affirmative practise begins by questioning heteronormative assumptions, by resituating oneself regarding their privileges and intersections, and by gaining knowledge on trans history.
Terms like “Western”, “universalist”, or “generalised”, mentioned in several points above, should be subject to scrutiny. It is careless to talk about standardisation without acknowledging the intrinsic diversification of practices, cares and bodily representations that often remain hidden. To deny it is, as Annemarie Mol stresses, a “form of internal colonisation” (2008, p. 6).
Thus, to explore the divergences in meanings and structures inside the Western tradition of care is to make a step against homogenising tendencies, which may seem unwavering but require particular attention. Some situated attainments can be reflected in psychological guidelines and reports (APA, 2015; BPS, 2019). However, more awareness is required, in order to contest universalist criteria of gender dysphoria with locatable and non-stigmatising models of body expression and variation.
Situated knowledge gained through local practices, sharing environments and horizontal therapeutic alliances can help MHPs overcome their gender biases and view TGNC people inside a context —involving culture, family, work, housing, resources, healthcare and special needs—. A deductive project of “trans ontology” is gradually replaced by relational perspectives, where people’s gender identity and expression are highly interrelated with the surroundings and the situational dynamics. This model of cultural competence offers psychologists “new” opportunities of accompaniment, through active listening, constant feedback, and authentic sharing. Instead of delineating a centre-versusperiphery model of counselling practice with TGNC people, a discovery of intersections, particularities and interactions between different “provincial” models seems more advantageous (Shamdasani, 2018).
Similarly, TGNC experiences are expected to vary worldwide, for resources, protocols, health systems, professional practices, psychological knowledge and gender norms vary enormously as well (Wylie et al., 2016). If gender affirmation adheres to standardisation and not to personal narratives of gender, it keeps following biomedical models (Johnson, 2016). Instead of creating a global, “-etic”, one-size-fits-all model of transition, prone to silencing and unnecessary labelling, psychologists are more likely to provide accurate services if they opt for listening to what people narrate about their individual contexts and needs, through their own voices.
Critical epistemological tools by STS Studies, interdisciplinary approaches, lay and activist coalitions, as well as inclusive and affirmative approaches in psychotherapy, form prominent methodological weapons of debating gender biases in psychological practice, urging psychologists to review their own stereotypes, to re-read their protocols and to revise their criteria (Hendricks and Testa, 2012). They do this through validating situated, “-emic” awareness as legit, and through questioning the well-established hierarchies described above. Careful cross-cultural adaptation of competences, considering linguistic variations and divergent manifestations of nonconformity in culture, prevents the imposition of terminologies that overshadow local, embodied ways of understanding TGNC.
When TGNC people are demanded to first resolve their “co-occurring” or “comorbid” mental health issues in order to gain access to bodily transition, ableist biases are projected upon them. The argument that they do not have complete mental capacity to make their own choices perpetuates their dependence upon diagnostic manuals (shuster, 2019). Therapeutic spaces permissive of authentic expression resignify this distress. By highlighting embodied knowledge, depathologising psychological practice unlocks the possibility for TGNC people to assume the therapeutic role themselves (Shipman and Martin, 2017). Their mediated narratives integrate the affirmative model through a new, hybrid expertise.
Discussion
The current study wished to critically relocate three major psychotherapeutic models for TGNC people in the universal-situated dichotomy. The main purpose was to claim that, even though depathologisation of gender diversity seems to break with standardised gender criteria, it risks over-generalisation if it ignores intersectional knowledge and cultural competence. To advocate for more authentic encounters in psychotherapeutic practice after the ICD-11 revision may seem insignificant, since psychologists’ role has been lessened. Nevertheless, it strategically calls for new practice ideals that emphasise lived experience.
Wholly, assessment and therapy with TGNC people corroborate a history of systematic pressure to follow indications, guidelines and protocols intended for binary gender norms. In a quest to diversify such procedures, however, we might witness how, the more we “undo” gender, the more we also “redo” it, paraphrasing Laurel Westbrook and Kristen Schilt (2014). This paradox needs to be addressed through constant revision of our personal biases.
Narrative shifts concerning identities are hard to delineate, since they cannot be corseted into clear chronological periods. The described models may coexist in the same context, time period, even multidisciplinary team. Transgender people wishing to pass as cisgender, or wanting to undergo bodily operations, can and do co-exist in the same cultural contexts with nonbinary people that wish to keep their bodies intact and have no need to follow gender stereotypes. The same observation is applicable to cross-cultural manifestations of transgender issues: it is hard to distinguish between universalist and local practices, in social contexts where both can be equally represented.
Instead of opting for a relativist approach, a situated one is encouraged: as if in a case study, it is important to observe the context in which each TGNC experience is developed, because sometimes, standardisation restricts MHPs in offering personalised services. Despite that, not all psychologists agree in the use of guidelines, protocols and questionnaires. Not all guidelines for psychologists over-simplify or over-generalise; meaning to have a broad coverage, several attempts are indeed respectful of particularities, intersections and exceptions.
Albeit theoretically, I have ventured a comparison between what seems to be an outmoded tradition of gender determination and its deconstruction. Similarly, I wished to highlight that Western psychology should not be understood as a robust entity. There are many intrinsic contradictions and alternative paths that need to be unravelled in the process of de-universalising the psychological views of gender. Provincialisation (Shamdasani, 2018) or localisation (Gerritse et al., 2018) can aid the process of better contextualising this culture of suspicion TGNC people and psychologists have been historically immersed into. Situated studies on the negative attitudes and reluctance of MHPs, along with suggestions for adequate training (see, for instance, López-Sáez et al., 2020, on the matter) are also highly urged.
Limitations
The present analysis draws heavily on previous designs. It is far from exhaustive, since it is not interested in capturing all possible implications of how dominant discourses on gender interact with transgender identities. For a more comprehensive view of the effects of those discursive mechanisms, longitudinal, cross-sectional and cross-cultural data would be necessary, both on expert and on lay level.
Critically informing on gaps in counselling and psychotherapy is also replete with methodological issues. Studies do not reckon information on the therapeutic alliance using the same tools, nor do they value confidentiality uniformly. Each therapeutic school manages different notions and techniques; therefore the application of the models outlined above is also expected to vary accordingly. Drawing upon situated STS epistemologies, cross-cultural psychology and gender studies literature, my paper covered a limited time period after the ICD revision, which has not yet been fully integrated. Future contributions should pay attention to how knowledge on the matter is produced inside the psychotherapeutic alliance, what implications it has for TGNC people, and how it is processed by research and scholarship.
Acknowledgements
A preliminary, oral draft of this paper was presented in May 2020, at the Conference Turning Points: Interpreting the past, explaining the present and imagining the future, organised by the London Centre for Interdisciplinary Research. Part of the analysis was presented as a poster at the PRISMA Conference, in November 2020. I would like to thank my thesis supervisors, Eulalia Pérez Sedeño and Dau García Dauder, for their revisions and overall support. I would also like to express my gratitude to the reviewers for their corrections, to all the members of the EPHYCUBE Project, as well as to Konstantinos D. Karatzas, Miquel Missé, Elena-Olga Christidi, and the PRISMA Association, for their insights, discussions and creative influence.
References
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Author.
American Psychological Association (2015). Guidelines for psychological practice with transgender and gender nonconforming people. American Psychologist, 70(9), 832-864. https://doi.org/10.1037/a0039906
Athanasiou, Athena & Butler, Judith (2013). Dispossession: The performative in the political. Polity.
Bauer, Greta; Hammond, Rebecca; Travers, Robb; Kaay, Matthias; Hohanadel, Karin & Boyce, Michelle (2009). “I don’t think this is theoretical; this is our lives”: How erasure impacts health care for transgender people. Journal of the Association of Nurses in AIDS Care, 20(5), 348-361. https://doi.org/10.1016/j.jana.2009.07.004
Benson, Kristen (2013). Seeking support: Transgender client experiences with mental health services. Journal of Feminist Family Therapy, 25(1), 17-40. https://doi.org/10.1080/08952833.2013.755081
Billard, Thomas (2019). “Passing” and the Politics of Deception: Transgender Bodies, Cisgender Aesthetics, and the Policing of Inconspicuous Marginal Identities. In Tony Docan-Morgan (Ed.), Palgrave Handbook of Deceptive Communication (pp. 463-477). Palgrave Macmillan.
Billings, Dwight & Urban, Thomas (1982). The socio-medical construction of transsexualism: An interpretation and critique. Social Problems, 29(3), 266-282.
Bockting, Walter (2008). Psychotherapy and the real-life experience: From gender dichotomy to gender diversity. Sexologies, 17, 211-224. https://doi.org/10.1016/j.sexol.2008.08.001
Bockting, Walter; Robinson, Beatrice; Benner, A. & Scheltema, K. (2004). Patient satisfaction with transgender health services. Journal of Sex & Marital Therapy, 30(4), 277-294. https://doi.org/10.1080/00926230490422467
British Psychological Society (2019). Guidelines for psychologists working with gender, sexuality and relationship diversity. British Psychological Society.
Burckell, Lisa & Goldfried, Marvin (2006). Therapist qualities preferred by sexualminority individuals. Psychotherapy: Theory, Research, Practice, Training, 43(1), 32-49. https://doi.org/10.1037/0033-3204.43.1.32
Butler, Judith (2010). Prólogo: Transexualidad, transformaciones. En Miquel Missé & Gerard Coll-Planas (Eds.), El género desordenado: Críticas en torno a la patologización de la transexualidad (pp. 1-4). Egales.
Campbell, Nancy (2009). Reconstructing science and technology studies: Views from feminist standpoint theory. Frontiers: A Journal of Women Studies, 30(1), 1-29. https://doi.org/10.1353/fro.0.0033
Carroll, Lynne & Gilroy, Paula (2002). Transgender issues in counselor preparation. Counselor Education & Supervision, 41, 233-242. https://doi.org/10.1002/j.1556-6978.2002.tb01286.x
Castro Peraza, Mª Elisa; García Acosta, Jesús; Delgado, Naira; Pedromo Hernández, Ana María; Sosa Álvarez, María Inmaculada; Llabrés Solé, Rosa & Lorenzo Rocha, Nieves (2019). Gender identity: The human right of depathologization. International Journal of Environmental Research and Public Health, 16(6), 978. https://doi.org/10.3390/ijerph16060978
Chavez Korell, Shannon & Lorah, Peggy (2007). An overview of affirmative psychotherapy and counseling with transgender clients. In Kathleen Bieschke, Ruperto Perez & Kurt DeBord (Eds.), Handbook of counseling and psychotherapy with lesbian, gay, bisexual, and transgender clients (pp. 271-288). American Psychological Association.
Clark, Dawn & Loewenthal, Del (2015). Counselling psychology. In Christina Richards & Meg John Barker (Eds.), The Palgrave handbook of the psychology of sexuality and gender (pp. 280-299). Palgrave MacMillan.
Denny, Dallas (2004). Changing models of transsexualism. Journal of Gay & Lesbian Psychotherapy, 8(1-2), 25-40. https://doi.org/10.1300/J236v08n01_04
Doan, Petra (2010). The tyranny of gendered spaces: Reflections from beyond the gender dichotomy. Gender, Place & Culture: A Journal of Feminist Geography, 17(5), 635-654. https://doi.org/10.1080/0966369X.2010.503121
Drescher, Jack (2007). I’m your handyman: A history of reparative therapies. In Ariel Shidlo, Michael Schroeder & Jack Drescher (Eds.), Sexual conversion therapy: Ethical, clinical and research perspectives (pp. 5-24). The Haworth Medical Press.
Drescher, Jack (2013). Controversies in gender diagnoses. LGBT Health, 1(1), 9-13. https://doi.org/10.1089/lgbt.2013.1500
Egan, Susan & Perry, David (2001). Gender identity: A multidimensional analysis with implications for psychosocial adjustment. Developmental Psychology, 37(4), 451-463. https://doi.org/10.1037/0012-1649.37.4.451
Ehrensaft, Diane (2012). From gender identity disorder to gender identity creativity: True gender self child therapy. Journal of Homosexuality, 59(3), 337-356. https://doi.org/10.1080/00918369.2012.653303
Fausto-Sterling, Anne (2000). Dueling dualisms. In Sexing the body: Gender politics and the construction of sexuality (pp. 1-29). Basic Books.
Fernández Garrido, Sam (2021). La clínica intersexual como “zona de contacto”: Binarismo sexual, saberes expertos y otras artesanías biológicas en la clínica española contemporánea. Tesis doctoral sin publicar, Universidad de Granada.
Freeman, Lauren & Stewart, Heather (2019). Epistemic microaggressions and epistemic injustices in clinical medicine. In Benjamin Serman & Stacey Goguen (Eds.), Overcoming epistemic injustice: Social and psychological perspectives (pp. 121-138). Rowman & Littlefield.
Gaebel, Wolfgang; Stricker, Johannes & Kerst, Ariane (2020). Changes from ICD-10 to ICD-11 and future directions in psychiatric classification. Dialogues in Clinical Neuroscience, 22(1), 7-15. https://doi.org/10.31887/DCNS.2020.22.1/wgaebel
García Dauder, Dau (2018). Pedagogías de la diversidad en salud: Diálogos entre activismos trans e intersex y disciplinas psi. En Teresa Climent Clemente & Marta Carmona Osorio (Eds.), Tranpsiquiatría: Abordajes queer en salud mental (pp. 100-142). Asociación Española de Neuropsiquiatría.
Garfinkel, Harold (1967/1991). Passing and the managed achievement of sexual status in an intersexed person, part 1. In Studies in ethnomethodology (pp. 116-185). Prentice-Hall.
Gerritse, Karl; Hartman, Laura; Antonides, Marte; Wensing-Kruger & et al. (2018). Moral challenges in transgender care: A thematic analysis based on a focused ethnography. Archives of Sexual Behavior, 47, 2319-2333. https://doi.org/10.1007/s10508-018-1287-3
Gherovici, Patricia (2017). Transgender psychoanalysis: A lacanian perspective on sexual difference. Routledge.
Gómez-Gil, Esther; Esteva de Antonio, Isabel; Fernández Rodríguez, María; Almaraz, Maricruz; Hurtado Murillo, Felipe; Gómez Balaguer, Marcelino; Asenjo Araque, Nuria; Mora Porta, Mireia; Halperin Rabinovich, Irene; Fernández García, Rosa, Montejo, Ángel & Grupo GIDSEEN (2020). Nuevos modelos de atención sanitaria para las personas transgénero en el sistema sanitario español: Demandas, controversias y reflexiones. Revista Española de Salud Pública, 94(16), 1-14.
Grzanka, Patrick & Miles, Joseph (2016). The problem with the phrase “intersecting identities”: LGBT affirmative therapy, intersectionality, and neoliberalism. Sexuality Research and Social Policy, 13(2), 371-389. https://doi.org/10.1007/s13178-016-0240-2
Halberstam, Jack (1998). Transgender butch: Butch/FTM border wars and the masculine continuum. GLQ: A Journal of Lesbian and Gay Studies, 4(2), 287-310.
Hausman, Bernice (1995). Changing sex: Transsexualism, technology, and the idea of gender. Duke University Press.
Hendricks, Michael & Testa, Rylan (2012). A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the minority stress model. Professional Psychology: Research & Practice, 43(5), 460-467. https://doi.org/10.1037/a0029597
Hines, Sally (2013). Gender diversity, recognition and citizenship. Palgrave MacMillan.
Iantaffi, Alex & Bockting, Walter (2011). Views from both sides of the bridge? Gender, sexual legitimacy, and transgender people’s experiences of relationships. Culture, Health & Sexuality, 13(3), 355-370. https://doi.org/10.1080/13691058.2010.537770
Israel, Tania; Gorcheva, Raya; Burnes, Theodore & Walther, William (2008). Helpful and unhelpful therapy experiences of LGBT clients. Psychotherapy Research, 18(3), 294-305. https://doi.org/10.1080/10503300701506920
Johnson, Austin (2016). Transnormativity: A new concept and its validation through documentary film about transgender men*. Sociological Inquiry, 86(4), 465-491. https://doi.org/10.1111/soin.12127
Latham, JR (2016). Trans men’s sexual narrative-practices: Introducing STS to trans and sexuality studies. Sexualities, 19(3), 347-368. https://doi.org/10.1177/1363460715583609
López-Sáez, Miguel & García Dauder, Dau (2020). Los test de masculinidad/feminidad como tecnologías psicológicas de control de género. Athenea Digital, 20(2), e2521, 1-30. https://doi.org/10.5565/rev/athenea.2521
López-Sáez, Miguel, García Dauder, Dau & Montero, Ignacio (2020). Correlate attitudes toward LGBT and sexism in Spanish psychology students. Frontiers in Psychology, 11(2063), 1-11. https://doi.org/10.3389/fpsyg.2020.02063
Lugones, María (2008). Colonialidad y género: Hacia un feminismo descolonial. In Walter Mingolo (Comp.), Género y descolonialidad (pp. 13-54). Del Signo.
Mason-Schrock, Douglas (1996). Transsexuals’ narrative construction of the “true self”. Social Psychology Quarterly, 59(3), 176-192.
McBee, Clare (2013). Towards a more affirming perspective: Contemporary psychodynamic practice with trans* and gender non-conforming individuals. Advocate’s Forum, 37-52. https://crownschool.uchicago.edu/sites/default/files/uploads/AdcovatesForum_2013_TowardsAMoreAffirmingPerspective.pdf
McLemore, Kevin (2014). Experiences with misgendering: Identity misclassification of transgender spectrum individuals. Self and identity, 14(1), 51-74. https://doi.org/10.1080/15298868.2014.950691
Missé, Miquel (2018). A la conquista del cuerpo equivocado. Egales.
Mizock, Lauren & Lundquist, Christine (2016). Missteps in psychotherapy with transgender clients: Promoting gender sensitivity in counseling and psychological practice. Psychology of Sexual Orientation and Gender Diversity, 3(2), 148-155. https://doi.org/10.1037/sgd0000177
Mol, Annemarie (2008). The logic of care: Health and the problem of patient choice. Taylor & Francis.
Nadal, Kevin; Skolnik, Avy & Wong, Yinglee (2012). Interpersonal and systemic microaggressions toward transgender people: Implications for counseling. Journal of LGBT Issues in Counseling, 6(1), 55-82. https://doi.org/10.1080/15538605.2012.648583
Occhino, Molly & Skewes, Lea (2020). Gatekeepers for gendersex norms: Trans (un)intelligibility and (il)legitimacy within the Danish healthcare system. NORA: Nordic Journal of Feminist and Gender Research, 28(4), 314-328, https://doi.org/10.1080/08038740.2020.1834450
Ortega Arjonilla, Esther; García Dauder, Dau; Gregori Flor, Nuria & Pérez Sedeño, Eulalia (2018). Practices and Knowledge: Philosophy of Biomedicine, Governance and Citizen Participation. In Belén Laspra & José Antonio López Cerezo (Eds.), Spanish philosophy of technology: Contemporary work from the Spanish speaking community (pp. 73-86). Springer.
O’ Shaughnessy, Tiffany & Speir, Zachary (2018). The state of LGBQ affirmative therapy clinical research: A mixed-methods systematic synthesis. Psychology of Sexual Orientation and Gender Diversity, 5(1), 82-98. https://doi.org/10.1037/sgd0000259
Pingitore, David; Scheffler, Richard; Sentell, Tetine & West, Joyce (2002). Comparison of psychiatrists and psychologists in clinical practice. Psychiatric Services, 53(8), 977-983. https://doi.org/10.1176/appi.ps.53.8.977
Raj, Rupert (2002). Towards a transpositive therapeutic model: Clinical competence in the effective support of transsexual and transgendered clients. International Journal of Transgenderism, 6(2), nn. pp.
Raun, Tobias (2014). Video blogging as a vehicle of transformation: Exploring the intersection between trans identity and information technology. International Journal of Cultural Studies, 20(10), 1-14. https://doi.org/10.1177/1367877913513696
Rood, Brian; Reisner, Sari; Surace, Francisco; Puckett, Jae; Maroney, Meredith & Pantalone, David (2016). Expecting rejection: Understanding the minority stress experiences of transgender and gender-nonconforming individuals. Transgender Health, 1(1), 151-164. https://doi.org/10.1089/trgh.2016.0012
Sennott, Shannon (2010). Gender disorder as gender oppression: A transfeminist approach to rethinking the pathologization of gender non-conformity. Women and Therapy, 34(1-2), 93-113. https://doi.org/10.1080/02703149.2010.532683
Serano, Julia (2016). Outspoken: A decade of transgender activism and trans feminism. Switch Hitter Press.
Shamdasani, Sonu (2018). Towards transcultural histories of psychotherapies. European Journal of Psychotherapy & Counselling, 20(1), 4-9, https://doi.org/10.1080/13642537.2018.1425111
Shipman, Daran & Martin, Tristan (2017). Clinical and supervisory considerations for transgender therapists: Implications for working with clients. Journal of Marital and Family Therapy, 45(1), 92-105. https://doi.org/10.1111/jmft.12300
shuster, stef (2019). Performing informed consent in transgender medicine. Social Science & Medicine, 226, 190-197. https://doi.org/10.1016/j.socscimed.2019.02.053
Spade, Dean (2006). Mutilating gender. In Susan Stryker & Stephen Whittle (Eds.), The transgender studies reader (pp. 315-332). Routledge.
Spanos, Cassandra; Grace, Julian; Leemaqz, Shalem; Brownhill, Adam; Cundill, Pauline; Locke, Peter; Wong, Peggy; Zajac, Jeffrey & Cheung, Ada (2020). The informed consent model of care for accessing gender-affirming hormone therapy is associated with high patient satisfaction. The Journal of Sexual Medicine, 18(1), 201-208. https://doi.org/10.1016/j.jsxm.2020.10.020
Stone, Sandy (1987/1991). The empire strikes back: A posttranssexual manifesto. In Kristina Straub & Julia Epstein (Eds.), Body Guards: The Cultural Politics of Gender Ambiguity (pp. 221-235). Routledge.
Suess, Amets (2020). Trans health care from a depathologization and human rights perspective. Public Health Reviews, 41(3), 1-17. https://doi.org/10.1186/s40985-020-0118-y
Tate, Charlotte (2014). Gender identity as a personality process. In Beverly Miller (Ed.), Gender identity: Disorders, developmental perspectives and social implications (pp. 1-22). Nova Science Publishers.
Tosh, Jemma (2016). Psychology and gender dysphoria: Feminist and transgender perspectives. Routledge.
Westbrook, Laurel & Schilt, Kristen (2014). Transgender people, gender panics, and the maintenance of the sex/gender/sexuality system. Gender & Society, 28(1), 32-57. https://doi.org/10.1177/0891243213503203
Wood, Wendy & Eagly, Alice (2015). Two Traditions of Research on Gender Identity. Sex Roles, 73, 461-473. https://doi.org/10.1007/s11199-015-0480-2
World Health Organization (2018). International statistical classification of diseases and related health problems (11th ed.). https://icd.who.int/
Wright, Talen; Candy, Bridget & King, Michael (2018). Conversion therapies and access to transition-related healthcare in transgender people: A narrative systematic review. BMJ Open, 8, 1-12. https://doi.org/10.1136/bmjopen-2018-022425
Wylie, Kevan; Knudson, Gail; Khan, Sharful; Bonierbale, Mireille; Watanyusakul, Suporn & Baral, Stefan (2016). Serving transgender people: Clinical care considerations and service delivery models in transgender health. The Lancet, 388(10042), 401-411. https://doi.org/10.1016/S0140-6736(16)00682-6
KONSTANTINOS ARGYRIOU
Cultural psychologist, PhD Candidate in Interdisciplinary Gender Studies at the Dpt. Of Science, Technology and Society of the Institute of Philosophy of the Spanish Na-tional Research Council (IFS/CSIC) and the Autonomous University of Madrid (UAM).
konstantinos.argyriou@cchs.csic.es
https://orcid.org/0000-0002-0578-7960
FUNDING
This research has been funded by the Spanish Ministry of Universities, under the Grant Formación de Profesorado Universitario (FPU17/03809). Part of the research also pertains to the Research Project I+D+i “Hybrid epistemologies: Bodies, biomet-rics and assemblages” (EPHYCUBE) (PID2019-105428RB-100) of the Spanish Ministry of Science.
ACKNOWLEDGEMENTS
A preliminary, oral draft of this paper was presented in May 2020, at the Confer-ence Turning Points: Interpreting the past, explaining the present and imagining the future, organised by the London Centre for Interdisciplinary Research. Part of the analysis was presented as a poster at the PRISMA Conference, in November 2020. I would like to thank my thesis supervisors, Eulalia Pérez Sedeño and Dau García Dauder, for their revisions and overall support. I would also like to express my gratitude to the reviewers for their corrections, to all the members of the EPHYCUBE Project, as well as to Konstantinos D. Karatzas, Miquel Missé, Elena-Olga Christidi, and the PRISMA Association, for their insights, discussions and creative in-fluence.
DISCLOSURE STATEMENTS
The author declares no potential conflict of interest.
FORMATO DE CITACIÓN
Argyriou, Konstantinos (2022). Trajectories towards affirmation: Gender identity in mental health services after the ICD-11. Quaderns de Psicologia, 24(2), e1821. https://doi.org/10.5565/rev/qpsicologia.1821
HISTORIA EDITORIAL
Recibido: 26-04-2021
1ª revisión: 03-09-2021
Aceptado: 08-10-2021
Publicado: 31-08-2022
_______________________________
1 The acronym TGNC (APA, 2015; Hendricks and Testa, 2012; McBee, 2013; Rood et al., 2016) permits an understanding of transgender that goes beyond the ongoing normalisation of the distinction between sex assigned at birth and current gender identity. In recent literature, it designates a wide variety of subjects and experiences such as transsexual, transgender, intersex, nonconforming, genderqueer, nonbinary, or polygender, among others. Its use wishes to assume the difficulties of encompassing both people who wish to undergo bodily interventions and people who transition only socially. Throughout the text, I use “TGNC”, “trans” and “gender diversity” interchangeably.